


Published: 19 May 2026. The English Chronicle Desk. The English Chronicle Online
The World Health Organization (WHO) recently issued a stark declaration, elevating the expanding Ebola crisis in Central Africa to a Public Health Emergency of International Concern (PHEIC). With the death toll in the Democratic Republic of Congo (DRC) and Uganda rapidly climbing past 131 amid more than 513 suspected cases, global health networks are scrambling.
To understand why this specific crisis is escalating at a “160 MPH clip,” it is critical to look beneath the terrifying headlines. Understanding what Ebola actually is reveals why stopping this particular outbreak has introduced a severe “resilience deficit” to international health protocols.

Ebola Virus Disease (EVD) is a severe, frequently fatal illness caused by an infection with a virus from the Orthoebolavirus genus. First identified in 1976 near the Ebola River in what is now the DRC, the virus is a zoonotic pathogen, meaning it originates in animals. Fruit bats are widely considered the natural reservoir host.
[Transmission Cycle of Ebola Virus: Fruit Bats/Wildlife -> Initial Human Spillover -> Human-to-Human via Bodily Fluids]
Unlike highly infectious respiratory diseases like COVID-19 or measles, Ebola is not airborne. It cannot travel through the air when someone coughs or sneezes. Instead, it spreads strictly through:
Direct Contact: Broken skin or mucous membranes coming into contact with the blood, secretions, organs, or other bodily fluids of an infected person.
Fomites: Surfaces, bedding, or clothing contaminated with these infectious fluids.
Post-Mortem Contact: Traditional burial practices involving direct physical contact with the deceased, whose viral loads remain highly potent.
Once inside the body, the virus attacks endothelial cells lining the blood vessels and systematically dismantles the immune system. This causes a “nasty” clinical progression that begins with generic symptoms like fever, severe headache, and muscle pain, before rapidly advancing to systemic vomiting, diarrhea, kidney failure, and internal and external hemorrhaging.
While the DRC has successfully managed multiple Ebola outbreaks over the past decade, the 2026 emergency presents an “asymmetric” nightmare for field epidemiologists, rendering traditional containment strategies largely ineffective.
The primary catalyst for the current “accountability rot” is the specific pathogen driving the infection: the Bundibugyo virus strain. There are four primary strains of Ebola known to affect humans, with the Zaire strain historically being the most common.
Because Zaire has dominated previous decades, almost all standard, rapid field tests deployed in remote African clinics are calibrated exclusively to detect Zaire. When the current outbreak ignited in the gold-mining hub of Mongbwalu in late April, initial samples “clinically” registered as negative. By the time advanced genomic sequencing at the INRB laboratory in Kinshasa identified the rare Bundibugyo strain on May 14, the virus had already spent weeks spreading undetected through informal healthcare networks.
In previous emergencies, health workers relied on the highly effective Ervebo vaccine to construct a protective shield around outbreaks using “ring vaccination” (vaccinating all contacts of an infected individual).
[Ring Vaccination Strategy: Confirmed Case -> Ring 1 (Close Contacts) -> Ring 2 (Contacts of Contacts)]
However, Ervebo is engineered strictly for the Zaire strain. Currently, there are no approved vaccines or specific therapeutics available for the Bundibugyo strain. Medical teams are forced to fight this outbreak using basic, supportive symptom management alone, bypassing the “milestone” pharmaceutical tools that saved thousands of lives during the 2018–2020 West Kivu epidemic.
The epicenter of the outbreak sits squarely within Ituri Province, a highly volatile region fractured by ongoing humanitarian crises and violent clashes between various armed factions, including the March 23 Movement.
Since early 2025, there have been dozens of documented attacks on local healthcare facilities. This pervasive insecurity creates a massive “resilience deficit” for contact tracers. Healthcare workers cannot safely enter rebel-controlled zones to monitor exposed individuals, creating an immediate chokepoint where chains of transmission completely vanish into unstable, highly mobile refugee populations.
Ebola is traditionally easiest to contain when it remains isolated in remote, deep-forest villages. The 2026 outbreak, however, hit highly connected commercial hubs almost immediately.
Confirmed cases have crossed international frontiers at a “160 MPH clip.” Infected travelers from Ituri have already triggered positive laboratory results in the Ugandan capital of Kampala, the major eastern DRC transit hub of Goma, and the political capital of Kinshasa. Goma’s subsequent closure of its border with Rwanda highlights the administrative friction now complicating humanitarian access.

The 2026 Bundibugyo surge proves that the international community can no longer rely on a static pandemic playbook. Without a functioning vaccine, and operating within a war zone, global health networks are facing an absolute crisis of containment.
“We have bypassed the ‘bottleneck’ of standard diagnostics, but we are facing an uphill battle against a strain we cannot vaccinate against,” a global health security analyst observed. Until security can be established for frontline tracers and experimental therapeutics are fast-tracked to the field, the “speechless determination” of isolated medical workers remains the only thin line defending the region from a major international disaster.
Related News:
 UK Must Act with Courage and Clarity on Israel-Palestine Conflict, Says Foreign Affairs Committee Report
UK Must Act with Courage and Clarity on Israel-Palestine Conflict, Says Foreign Affairs Committee Report
 Terence Stamp, ’60s British Film Legend and Star of Superman, Dies at 87
Terence Stamp, ’60s British Film Legend and Star of Superman, Dies at 87
 Hong Kong Summons UK and Australian Envoys Following Asylum Grants to Democracy Activists
Hong Kong Summons UK and Australian Envoys Following Asylum Grants to Democracy Activists
 Is the UK Ready to Put Boots on the Ground in Ukraine? Assessing Military Capacity and Challenges
Is the UK Ready to Put Boots on the Ground in Ukraine? Assessing Military Capacity and Challenges
 Channel Crossings Surge: Over 1,000 People Arrive in the UK in Small Boats in a Single Day
Channel Crossings Surge: Over 1,000 People Arrive in the UK in Small Boats in a Single Day
 Yvette Cooper Signals Global Momentum Towards Gaza Peace Deal Amid Humanitarian Crisis
Yvette Cooper Signals Global Momentum Towards Gaza Peace Deal Amid Humanitarian Crisis
 Chaos at Ibrox as Martin’s Rangers Era Comes to an End
Chaos at Ibrox as Martin’s Rangers Era Comes to an End
 Russia’s Latest Push to Win US Favors Shows Deep Desperation
Russia’s Latest Push to Win US Favors Shows Deep Desperation
 BBC to Apologise Over Edited Trump Speech Amid Backlash
BBC to Apologise Over Edited Trump Speech Amid Backlash
 Greene Pushes Epstein Files Amid Trump Fallout
Greene Pushes Epstein Files Amid Trump Fallout
 Zelenskyy Signs Fighter Jet Deal Amid Russian Drone Attacks
Zelenskyy Signs Fighter Jet Deal Amid Russian Drone Attacks
 Shadow Fleet at Sea: Europe’s Battle Against Illicit Oil Shipping
Shadow Fleet at Sea: Europe’s Battle Against Illicit Oil Shipping
 US Suspends Afghan Immigration After White House Shooting
US Suspends Afghan Immigration After White House Shooting
 ‘Extinct’ Antelope Returns to Sahara, Bringing Hope
‘Extinct’ Antelope Returns to Sahara, Bringing Hope
 Sydney Shark Attack Surge Shocks Australia Beaches
Sydney Shark Attack Surge Shocks Australia Beaches
 Portugal Election Delivers Socialist Win as Far Right Surges
Portugal Election Delivers Socialist Win as Far Right Surges
 Australian Families Leave Syrian Camp for Home
Australian Families Leave Syrian Camp for Home
 ‘I Would Scream in My Sleep’: Alawite Women from Syria Tell of Kidnap and Rape
‘I Would Scream in My Sleep’: Alawite Women from Syria Tell of Kidnap and Rape
 Snow and Rain Warnings as Cold Snap Continues in the UK
Snow and Rain Warnings as Cold Snap Continues in the UK
 Nine Arrested in France Over Death of Far‑Right Student
Nine Arrested in France Over Death of Far‑Right Student
 Indian University Kicked Out of AI Summit for Claiming Chinese Robot Dog as Its Own Invention
Indian University Kicked Out of AI Summit for Claiming Chinese Robot Dog as Its Own Invention
 Epstein Eyed Record Label Investment to Access Women, Files Suggest
Epstein Eyed Record Label Investment to Access Women, Files Suggest
 How Do You Modernise Mango Farming? India’s Growers Urged to Innovate as Climate Change Hits
How Do You Modernise Mango Farming? India’s Growers Urged to Innovate as Climate Change Hits
 Australian PM Says Former Prince Andrew Has Suffered ‘Extraordinary Fall’ but That Won’t Prompt Republic Referendum
Australian PM Says Former Prince Andrew Has Suffered ‘Extraordinary Fall’ but That Won’t Prompt Republic Referendum
 Farage Chagos Islands Row Sparks Fury
Farage Chagos Islands Row Sparks Fury
 Storm Hernando: Edinburgh Airport Flights Cancelled in US Travel Chaos
Storm Hernando: Edinburgh Airport Flights Cancelled in US Travel Chaos
 Ukraine Negotiator Reveals What It Feels Like Facing Russia
Ukraine Negotiator Reveals What It Feels Like Facing Russia
 Chad Shuts Border With Sudan in Bid to Stop Conflict Spreading
Chad Shuts Border With Sudan in Bid to Stop Conflict Spreading
 Drugs, Denial, Stigma: Fiji’s HIV Crisis Hits Children
Drugs, Denial, Stigma: Fiji’s HIV Crisis Hits Children
 Hilary Knight speaks out on Trump’s recent hockey remarks
Hilary Knight speaks out on Trump’s recent hockey remarks
 American Citizen Killed in Cuba Boat Shooting, U.S. Officials Say
American Citizen Killed in Cuba Boat Shooting, U.S. Officials Say
 Iran’s Regime Still Intact — Coming Days Will Test Its Survival
Iran’s Regime Still Intact — Coming Days Will Test Its Survival
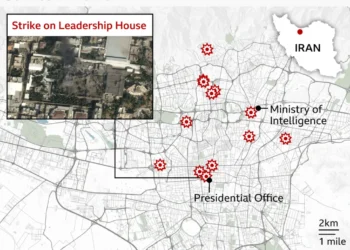 In Maps: Strikes Across Iran and the Middle East
In Maps: Strikes Across Iran and the Middle East
 Brit ‘in Good Spirits’ Amid Dubai Missile Attacks, Stranded but Safe
Brit ‘in Good Spirits’ Amid Dubai Missile Attacks, Stranded but Safe
 Civilian Deaths in Iran Pass 700 Amid Fear of Bombs and Regime Clampdown
Civilian Deaths in Iran Pass 700 Amid Fear of Bombs and Regime Clampdown
 ‘Every Day Feels Like a Month’: Iranians Describe Life Under ‘Constant’ US‑Israeli Strikes
‘Every Day Feels Like a Month’: Iranians Describe Life Under ‘Constant’ US‑Israeli Strikes
 Penny Wong silent on Australian crew in sub strike
Penny Wong silent on Australian crew in sub strike
 Finland Plans to Lift Decades‑Old Ban on Hosting Nuclear Weapons
Finland Plans to Lift Decades‑Old Ban on Hosting Nuclear Weapons
 Trump Pressures Congress Over Save America Act
Trump Pressures Congress Over Save America Act
 Iran War Puts Trump at Political Risk Amid Rising Prices
Iran War Puts Trump at Political Risk Amid Rising Prices
 Goma Drone Attack Kills Three as Conflict Escalates
Goma Drone Attack Kills Three as Conflict Escalates
 Queensland Protest Laws Spark Free Speech Backlash
Queensland Protest Laws Spark Free Speech Backlash
 Trump Nato threats expose Iran strategy vacuum
Trump Nato threats expose Iran strategy vacuum
 Trump Facing Backlash from Epstein Survivors Over Files
Trump Facing Backlash from Epstein Survivors Over Files
 UK Forces Ready to Seize Russian Shadow Fleet Vessels
UK Forces Ready to Seize Russian Shadow Fleet Vessels
 Trump Considers Military Operation to Seize Iran’s Uranium
Trump Considers Military Operation to Seize Iran’s Uranium
 “It Ends With Trial”: Judge Tosses Blake Lively’s Sexual Harassment Claims Against Justin Baldoni
“It Ends With Trial”: Judge Tosses Blake Lively’s Sexual Harassment Claims Against Justin Baldoni
 The Banbridge Rescue: 300 Sheep Saved from Massive Hay Shed Inferno
The Banbridge Rescue: 300 Sheep Saved from Massive Hay Shed Inferno
 Report Says Pezzullo Acted ‘Recklessly’ in Dealings
Report Says Pezzullo Acted ‘Recklessly’ in Dealings
 Oil and Diplomacy: Russian Refineries Burn as Zelenskyy Secures Middle East Shield
Oil and Diplomacy: Russian Refineries Burn as Zelenskyy Secures Middle East Shield
 Electric Shock: Australians Buy Record Number of New EVs as Fuel Crisis Bites
Electric Shock: Australians Buy Record Number of New EVs as Fuel Crisis Bites
 The Suffocating Silhouette: Why Metal’s Mask Trend is Turning Deadly
The Suffocating Silhouette: Why Metal’s Mask Trend is Turning Deadly
 The Great Chokehold: Why the Strait of Hormuz is the Epicenter of the 2026 Crisis
The Great Chokehold: Why the Strait of Hormuz is the Epicenter of the 2026 Crisis
 Moldova River Crisis Exposes War’s Hidden Cost
Moldova River Crisis Exposes War’s Hidden Cost
 Tragedy Strikes Outside Melbourne Comic Con
Tragedy Strikes Outside Melbourne Comic Con
 The Fog of War and the Ticker Tape: Suspicious Trades Rile Washington
The Fog of War and the Ticker Tape: Suspicious Trades Rile Washington
 ‘A Fragile Calm’: Oil Prices Dip as Trump Extends Iran Ceasefire, But Blockade Holds Firm
‘A Fragile Calm’: Oil Prices Dip as Trump Extends Iran Ceasefire, But Blockade Holds Firm
 Justice and Deceit: High Court Convicts Woman in Hong Kong Blackmail Plot
Justice and Deceit: High Court Convicts Woman in Hong Kong Blackmail Plot
 Judicial Whiplash: Virginia Court Pauses Redistricting 24 Hours After Public Vote
Judicial Whiplash: Virginia Court Pauses Redistricting 24 Hours After Public Vote
 “Industrial-Scale Extraction”: White House Memo Accuses China of Mass AI Theft
“Industrial-Scale Extraction”: White House Memo Accuses China of Mass AI Theft
 Beyond the Swoosh: Anta Sports Overtakes Rivals to Become Global Top Three
Beyond the Swoosh: Anta Sports Overtakes Rivals to Become Global Top Three
 “Three-Wheeled Triumph”: Mayor of Erewash Completes 2,000-Mile European Charity Run
“Three-Wheeled Triumph”: Mayor of Erewash Completes 2,000-Mile European Charity Run
 Capitalism ‘Suicidal’, Warns Petro at Climate Summit
Capitalism ‘Suicidal’, Warns Petro at Climate Summit
 Tragedy in the Red Centre: Outback Search Ends in Discovery of Missing Girl’s Body
Tragedy in the Red Centre: Outback Search Ends in Discovery of Missing Girl’s Body
 The Silent Scythe: How the Iran War is “Starving” Asian Paddy Fields Before the Harvest
The Silent Scythe: How the Iran War is “Starving” Asian Paddy Fields Before the Harvest
 “An Endurance Test for the Mind”: British Couple Sentenced to 10 Years in Tehran
“An Endurance Test for the Mind”: British Couple Sentenced to 10 Years in Tehran
 US to Escort Trapped Ships Through the Strait of Hormuz
US to Escort Trapped Ships Through the Strait of Hormuz
 Premier League drama defines crucial weekend
Premier League drama defines crucial weekend
 “The Pivot to Pakistan”: Trump Pauses ‘Project Freedom’ in Hormuz Amid Iran Deal Hopes
“The Pivot to Pakistan”: Trump Pauses ‘Project Freedom’ in Hormuz Amid Iran Deal Hopes
 “The New Silk Road”: India and Vietnam Forge Strategic Maritime Alliance to Counter Regional Volatility
“The New Silk Road”: India and Vietnam Forge Strategic Maritime Alliance to Counter Regional Volatility
 “The Digital Frontier”: Scotland’s Papers Grapple with AI Harassment and ‘Mortgage Bottlenecks’
“The Digital Frontier”: Scotland’s Papers Grapple with AI Harassment and ‘Mortgage Bottlenecks’
 “The Local Gavel”: Polls Open Across Hampshire and Isle of Wight in Delayed ‘Milestone’ Vote
“The Local Gavel”: Polls Open Across Hampshire and Isle of Wight in Delayed ‘Milestone’ Vote
 “The Blue Light Intersection”: Seventeen-Year-Old Critically Injured in ‘Nasty’ Police Pursuit Crash
“The Blue Light Intersection”: Seventeen-Year-Old Critically Injured in ‘Nasty’ Police Pursuit Crash
 “The Fractured Frontier”: Sir John Curtice Declares the ‘Sacred’ Two-Party Era Over After ‘Milestone’ Results
“The Fractured Frontier”: Sir John Curtice Declares the ‘Sacred’ Two-Party Era Over After ‘Milestone’ Results
 US Awaits Iran Reply on New Ceasefire Proposal
US Awaits Iran Reply on New Ceasefire Proposal
 “The End of the Towel War?”: How Hotels are ‘Clinically’ Stopping the Sunbed Dash
“The End of the Towel War?”: How Hotels are ‘Clinically’ Stopping the Sunbed Dash
 Putin Signals War End as Russian Momentum Stalls
Putin Signals War End as Russian Momentum Stalls
 Philippine Senator Flees After Days Under Senate Siege
Philippine Senator Flees After Days Under Senate Siege
 High Street Crisis: Fears Grow Over Post Office Closures
High Street Crisis: Fears Grow Over Post Office Closures









{kind=link}