


Published: 30 December 2025. The English Chronicle Desk. The English Chronicle Online.
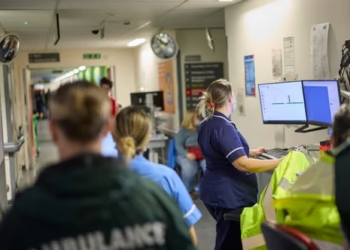
Emergency departments across the United Kingdom are facing an escalating crisis, as corridor care becomes an accepted reality rather than an emergency measure. Senior clinicians are warning that what was once viewed as unacceptable has now been normalised, placing patients at serious risk and pushing exhausted staff to breaking point. The comments come amid mounting evidence that long waits for hospital beds are contributing to thousands of avoidable deaths each year.
Dr Ian Higginson, president of the Royal College of Emergency Medicine, has described the situation as “big trouble” for the NHS, arguing that public outrage has failed to match the scale of harm being caused. He has warned that only a small number of hospitals have managed to avoid placing patients on trolleys in corridors, while the majority struggle daily with overcrowded emergency departments.

Corridor care, once considered a last resort during extreme pressure, has become so common that patients often expect it. According to Dr Higginson, many people arriving at A&E are no longer surprised to find themselves treated in hallways, storage spaces, or other unsuitable areas. This acceptance, he says, masks a profound failure of the healthcare system and undermines the quality and safety of care being delivered.
Medical staff working in these conditions report that providing effective treatment in corridors is nearly impossible. Privacy is compromised, infection risks increase, and critical monitoring becomes more difficult. Doctors and nurses are forced to make rapid decisions in crowded, noisy environments, often without access to essential equipment. Dr Higginson has stressed that clinicians simply cannot deliver safe and dignified care under such circumstances.
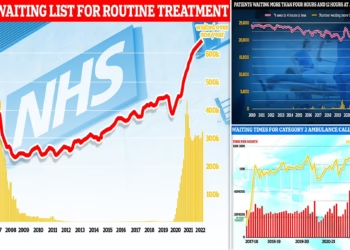
Earlier this year, the Royal College of Emergency Medicine released estimates suggesting that more than 16,600 patient deaths were linked to excessively long waits in A&E for hospital beds during the previous year. This equates to around 320 deaths every week, a figure that has shocked many within the profession but has yet to provoke decisive action at the highest political level.
Dr Higginson has drawn stark comparisons to other public safety disasters. He argued that if similar numbers of people were dying annually in transport accidents, there would be immediate national outrage and urgent reform. The lack of comparable reaction to A&E-related deaths, he believes, reflects a dangerous desensitisation to suffering within the health system.
Further analysis published earlier this month revealed that nearly one in five patients treated in UK emergency departments during March were cared for in so-called escalation areas. These areas include corridors and other non-clinical spaces not designed for patient treatment. Dr Higginson suspects that the situation has since worsened, mirroring broader signs of deterioration across the NHS.
The findings highlight how winter pressures, staff shortages, and delayed discharges combine to overwhelm hospitals. As beds remain occupied by patients who cannot be safely discharged, emergency departments become bottlenecks, forcing new arrivals to wait hours or even days for admission.
In December, Health Secretary Wes Streeting pledged to end corridor care in hospitals in England by the next general election, if not sooner. While the commitment has been welcomed, frontline clinicians remain cautious, noting that similar promises have been made before without lasting change. They argue that eliminating corridor care will require sustained investment and systemic reform rather than short-term fixes.
Dr Higginson has criticised what he sees as an overemphasis on quick, inexpensive solutions. Efforts to redirect patients away from hospitals, he said, may help at the margins but do not address the underlying causes of overcrowding. He insists that the crisis is solvable, but only with sufficient political will and a willingness to confront uncomfortable truths.
At the heart of the problem, he argues, is hospital inefficiency driven by chronic underfunding and workforce shortages. Increasing staffed bed capacity, improving patient flow, and strengthening community and social care services are essential steps. Without these changes, patients who are medically fit to leave hospital remain stuck, preventing others from being admitted from A&E.
The human cost of the crisis extends beyond patients to the staff caring for them. Many emergency clinicians describe being “run ragged,” working long shifts under relentless pressure. Burnout, moral injury, exhaustion, and symptoms consistent with post-traumatic stress disorder are increasingly reported among healthcare workers. Dr Higginson has warned that failing to improve conditions risks driving experienced staff out of the profession altogether.
Official NHS figures underscore the scale of the challenge. In November alone, more than 50,000 people in England waited over 12 hours in A&E from the decision to admit them to the point of being given a hospital bed. For many, these waits occurred in corridors, where basic comfort and dignity are difficult to maintain.

NHS England has acknowledged that such delays are unacceptable. A spokesperson said the organisation is working to free up beds by accelerating discharges for patients who are medically fit and expanding access to community-based care. This winter, productivity specialists and regional experts have been deployed to support hospitals in reducing corridor care and improving patient experience.
The Department of Health and Social Care has also conceded that corridor care is undignified and unacceptable. A spokesperson said the government inherited a difficult situation but remains determined to bring the practice to an end. Officials point to signs of recovery, including improvements in four-hour A&E performance and faster ambulance response times for life-threatening conditions.
However, critics argue that these improvements are fragile and unevenly distributed. They warn that focusing on headline targets risks obscuring the lived reality of patients waiting in unsuitable spaces. For those experiencing pain, fear, or confusion in crowded corridors, assurances of future reform offer little immediate comfort.
As winter continues to place intense strain on the NHS, the debate over corridor care has become a symbol of wider systemic failure. Clinicians like Dr Higginson insist that accepting the practice as normal is not only dangerous but morally wrong. They argue that public awareness and political urgency must match the severity of the harm being caused.
The coming months will test whether pledges to end corridor care translate into meaningful change. For now, emergency departments remain on the frontline of a crisis that many believe has been allowed to deepen for too long. The question facing policymakers is whether they are prepared to act decisively before normalisation turns into tragedy.
Related News:
 Concerns Mount Over Accuracy of At-Home Health Tests as Study Calls for Stricter Regulation
Concerns Mount Over Accuracy of At-Home Health Tests as Study Calls for Stricter Regulation
 NHS Under Pressure: Waiting Times Soar as Staffing Crisis Deepens
NHS Under Pressure: Waiting Times Soar as Staffing Crisis Deepens
 The Ketamine Crisis in the UK is a Silent Epidemic Leaving Users with Lifelong Pain
The Ketamine Crisis in the UK is a Silent Epidemic Leaving Users with Lifelong Pain
 UK Launches World-First Gonorrhoea Vaccine Amid Record Infection Surge
UK Launches World-First Gonorrhoea Vaccine Amid Record Infection Surge
 Woman Warned She Might Need Leg Amputation to Survive After Liquid Brazilian Butt Lift
Woman Warned She Might Need Leg Amputation to Survive After Liquid Brazilian Butt Lift
 AI Tools Used by English Councils Found to Downplay Women’s Health Issues, Raising Concerns Over Gender Bias in Care
AI Tools Used by English Councils Found to Downplay Women’s Health Issues, Raising Concerns Over Gender Bias in Care
 Cats Develop Dementia Similarly to Humans, Study Finds
Cats Develop Dementia Similarly to Humans, Study Finds
 Appalling Rise in Pharmacy Crimes: Staff Face Increasing Theft and Aggression
Appalling Rise in Pharmacy Crimes: Staff Face Increasing Theft and Aggression
 Alarming rise in abusive teen relationships in the UK sparks urgent warnings
Alarming rise in abusive teen relationships in the UK sparks urgent warnings
 Learner Drivers to Face CPR and Defibrillator Questions in New Theory Tests
Learner Drivers to Face CPR and Defibrillator Questions in New Theory Tests
 Inquest Finds Agency Worker Failings Led to Unlawful Death of Vulnerable 14-Year-Old
Inquest Finds Agency Worker Failings Led to Unlawful Death of Vulnerable 14-Year-Old
 UK Patients Face Steep Price Rise for Weight-Loss Drug Mounjaro
UK Patients Face Steep Price Rise for Weight-Loss Drug Mounjaro
 Shocking Rise in Children’s Exposure to Violent Online Pornography Raises Alarm
Shocking Rise in Children’s Exposure to Violent Online Pornography Raises Alarm
 Baby Food Manufacturers Given 18 Months to Improve Nutrition and Labelling
Baby Food Manufacturers Given 18 Months to Improve Nutrition and Labelling
 Why E-Bikes and E-Scooters Are Making Streets a ‘Nightmare’ for Blind People
Why E-Bikes and E-Scooters Are Making Streets a ‘Nightmare’ for Blind People
 Millions in the UK at Higher Risk of Heart Failure and Stroke Due to Air Pollution, Study Warns
Millions in the UK at Higher Risk of Heart Failure and Stroke Due to Air Pollution, Study Warns
 Norfolk Hospital Ranked Worst in England as NHS League Tables Return
Norfolk Hospital Ranked Worst in England as NHS League Tables Return
 NHS Trials £100 Blood Test That Could Revolutionise Alzheimer’s Diagnosis
NHS Trials £100 Blood Test That Could Revolutionise Alzheimer’s Diagnosis
 More Than Half of UK Births Now Involve Medical Intervention
More Than Half of UK Births Now Involve Medical Intervention
 UK Graduates in Healthcare Report Highest Satisfaction with Degree Choices
UK Graduates in Healthcare Report Highest Satisfaction with Degree Choices
 NHS ‘Toxic Culture’ Risks Harm to Mothers and Babies, Health Leader Warns
NHS ‘Toxic Culture’ Risks Harm to Mothers and Babies, Health Leader Warns
 Systemic Racism in Maternity Care Continues to Endanger Black Women in England, MPs Warn
Systemic Racism in Maternity Care Continues to Endanger Black Women in England, MPs Warn
 One in Three GPs in England Do Not Work in NHS, Raising Concerns Over Access to Care
UK Doctors Guilty of Sexual Misconduct Continue Practising Amid Weak Sanctions, Research Finds
One in Three GPs in England Do Not Work in NHS, Raising Concerns Over Access to Care
UK Doctors Guilty of Sexual Misconduct Continue Practising Amid Weak Sanctions, Research Finds
 Private Psychology Costs Surge in UK as Practitioners Turn Away Clients Amid Record Demand
Private Psychology Costs Surge in UK as Practitioners Turn Away Clients Amid Record Demand
 Heavy Drinkers Lead Growth in Non-Alcoholic and Low-Alcohol Market
Heavy Drinkers Lead Growth in Non-Alcoholic and Low-Alcohol Market
 Omeprazole Alert: NHS Issues Guidance on Safe Use for Heartburn and Indigestion
Omeprazole Alert: NHS Issues Guidance on Safe Use for Heartburn and Indigestion
 Starmer Unveils Plan for NHS “Online Hospital” to Tackle Waiting Lists
Starmer Unveils Plan for NHS “Online Hospital” to Tackle Waiting Lists
 Tragic Death Strikes Half-Marathon in Stoke-on-Trent: Runner Dies Shortly After Crossing Finish Line
Tragic Death Strikes Half-Marathon in Stoke-on-Trent: Runner Dies Shortly After Crossing Finish Line
 Call to Allow ‘Safe and Effective’ At-Home Abortions Up to 12 Weeks in the UK
Call to Allow ‘Safe and Effective’ At-Home Abortions Up to 12 Weeks in the UK
 Questions Remain as Rugby Legend Lewis Moody Faces Motor Neurone Disease Diagnosis
Questions Remain as Rugby Legend Lewis Moody Faces Motor Neurone Disease Diagnosis
 Eligibility Confusion Over COVID Vaccination Leaves Pharmacies Struggling Across the UK
Eligibility Confusion Over COVID Vaccination Leaves Pharmacies Struggling Across the UK
 Majority of UK Men Would Opt for Prostate Cancer Screening, Survey Finds
Majority of UK Men Would Opt for Prostate Cancer Screening, Survey Finds
 Scientists Announce First Potentially Accurate Blood Test for Chronic Fatigue Syndrome
Scientists Announce First Potentially Accurate Blood Test for Chronic Fatigue Syndrome
 NHS Facilities Staff Vote to Strike Over Pay Discrimination
NHS Facilities Staff Vote to Strike Over Pay Discrimination
 Survey Shows Most GPs Rushing Appointments
Survey Shows Most GPs Rushing Appointments
 NHS Staff Strike Over £30m Pay Discrimination Claim
NHS Staff Strike Over £30m Pay Discrimination Claim
 Ambulance Worker Fired After Flinging Amputee from Wheelchair and Offering Bribe
Ambulance Worker Fired After Flinging Amputee from Wheelchair and Offering Bribe
 Women Challenge Meta Over Targeted Ads After Miscarriage
Women Challenge Meta Over Targeted Ads After Miscarriage
 Mum’s Final Wish: Donating Her Body to Science
Mum’s Final Wish: Donating Her Body to Science
 Genetic Tests May Predict Return of Blood Cancer
Genetic Tests May Predict Return of Blood Cancer
 UK Woman Becomes Longest Survivor of Heart-Lung Transplant
£18 Prostate Cancer Test Could Save Thousands of Lives
UK Woman Becomes Longest Survivor of Heart-Lung Transplant
£18 Prostate Cancer Test Could Save Thousands of Lives
 Thousands in the UK sue Johnson & Johnson over alleged talcum powder, linked to cancer
Thousands in the UK sue Johnson & Johnson over alleged talcum powder, linked to cancer
 Pregnant Women in England Face Rising Risk of Severe Birth Injury
Pregnant Women in England Face Rising Risk of Severe Birth Injury
 ‘Game-Changing’ HIV Prevention Jab Set for NHS Approval
‘Game-Changing’ HIV Prevention Jab Set for NHS Approval
 One in 12 Secondary Pupils Sent to Isolation Weekly
One in 12 Secondary Pupils Sent to Isolation Weekly
 M&S and Morrisons Lead Christmas Supermarket Taste Test
New Prostate Cancer Drug Set to Halve Death Risk in England
M&S and Morrisons Lead Christmas Supermarket Taste Test
New Prostate Cancer Drug Set to Halve Death Risk in England
 UK Health Leaders Push for Urgent Tobacco & Vape Bill
UK Health Leaders Push for Urgent Tobacco & Vape Bill
 Man Trapped in Quicksand Rescued in Dramatic Coastal Rescue
Man Trapped in Quicksand Rescued in Dramatic Coastal Rescue
 Hospice Cuts Raise Alarm Across England Amid Funding Crisis
Hospice Cuts Raise Alarm Across England Amid Funding Crisis
 Celebrities and Charities Demand UK Government Act on Child Poverty
Celebrities and Charities Demand UK Government Act on Child Poverty
 Experts Warn on Home Birth Risks, Call for Skilled Midwives
Experts Warn on Home Birth Risks, Call for Skilled Midwives
 Experts Urge Legal Right to Timely Cancer Care
Experts Urge Legal Right to Timely Cancer Care
 Patients to Test Health at Home to Ease NHS Winter Pressure
Patients to Test Health at Home to Ease NHS Winter Pressure
 London’s Childlessness Crisis: Schools Closing as Families Shrink
London’s Childlessness Crisis: Schools Closing as Families Shrink
 North Sea oil workers must lose weight or face job loss
North Sea oil workers must lose weight or face job loss
 Crisis charity to become landlord amid UK housing emergency
Crisis charity to become landlord amid UK housing emergency
 Shouting Works Best to Deter Gulls, UK Study Finds
Shouting Works Best to Deter Gulls, UK Study Finds
 Reeves rejects £1bn plea for NHS redundancy payouts
Reeves rejects £1bn plea for NHS redundancy payouts
 Leading doctors issue warning amid ‘bad’ flu season
Leading doctors issue warning amid ‘bad’ flu season
 Stroke Patient Mistaken for Drunk, Care Delayed
Stroke Patient Mistaken for Drunk, Care Delayed
 UK launches major AI drive to fight deadly superbugs
UK launches major AI drive to fight deadly superbugs
 ‘Traumatic Wait’: Northern Ireland Women Face Breast Cancer Delays
‘Traumatic Wait’: Northern Ireland Women Face Breast Cancer Delays
 Welsh Government Christmas 2020 Lockdown Criticised
Welsh Government Christmas 2020 Lockdown Criticised
 Coffins Now Too Large to Cremate Amid Rising Obesity Crisis
Coffins Now Too Large to Cremate Amid Rising Obesity Crisis
 NHS paediatric leave parents waiting months for answers
NHS paediatric leave parents waiting months for answers
 Five-Year-Old Dies After Rare Tonsil Surgery Complication
Five-Year-Old Dies After Rare Tonsil Surgery Complication
 Fibromyalgia Patients Struggle as NHS Fails to Provide Care
Fibromyalgia Patients Struggle as NHS Fails to Provide Care
 “Enough is Enough”: Local MP Vows to Fight Rainham Quarry Plans
“Enough is Enough”: Local MP Vows to Fight Rainham Quarry Plans
 More Patients Now Contacting GPs Online, Data Shows
More Patients Now Contacting GPs Online, Data Shows
 GPs Failing Frail Elderly: Only 1 in 6 Assessed – NAO
GPs Failing Frail Elderly: Only 1 in 6 Assessed – NAO
 NHS Maternity Failings Leave Families Traumatized, Investigation Finds
NHS Maternity Failings Leave Families Traumatized, Investigation Finds
 NHS braces for worst winter crisis amid rising flu cases
NHS braces for worst winter crisis amid rising flu cases
 Inquiry Launched into North-East NHS Trust Patient Deaths
Inquiry Launched into North-East NHS Trust Patient Deaths
 Ministers to back regulation of England’s funeral industry
Ministers to back regulation of England’s funeral industry
 Teen Nicotine Pouch Use Sparks Growing Health Alarm
Teen Nicotine Pouch Use Sparks Growing Health Alarm
 People in England’s Poorest Areas Face Higher Lung Health Emergencies
People in England’s Poorest Areas Face Higher Lung Health Emergencies
 AI Helps NHS Cut A&E Waiting Times This Winter
AI Helps NHS Cut A&E Waiting Times This Winter









{kind=link}